


 LOGIN
LOGIN

Clinicians are interested to know the association between a therapy and an outcome. In clinical trials and observational studies, we find these associations by reading their results that report relative risk (RR), odds ratio (OR), hazard ratio (HR) and 95% confidence interval (CI). The other term that is often read in the clinical articles is number needed to treat (NNT). We also encounter terms such as relative difference, absolute difference, risk difference (RD), relative risk reduction (RRR) and absolute risk reduction (ARR) during journal clubs and clinical epidemiological courses or workshops. What do all these terms mean? How do we interpret them? In what ways can we apply them to clinical practice? In this OE Original, we present 5 quick tips that help you interpret these measures for dichotomous outcomes.
Anatomy of a Results Table
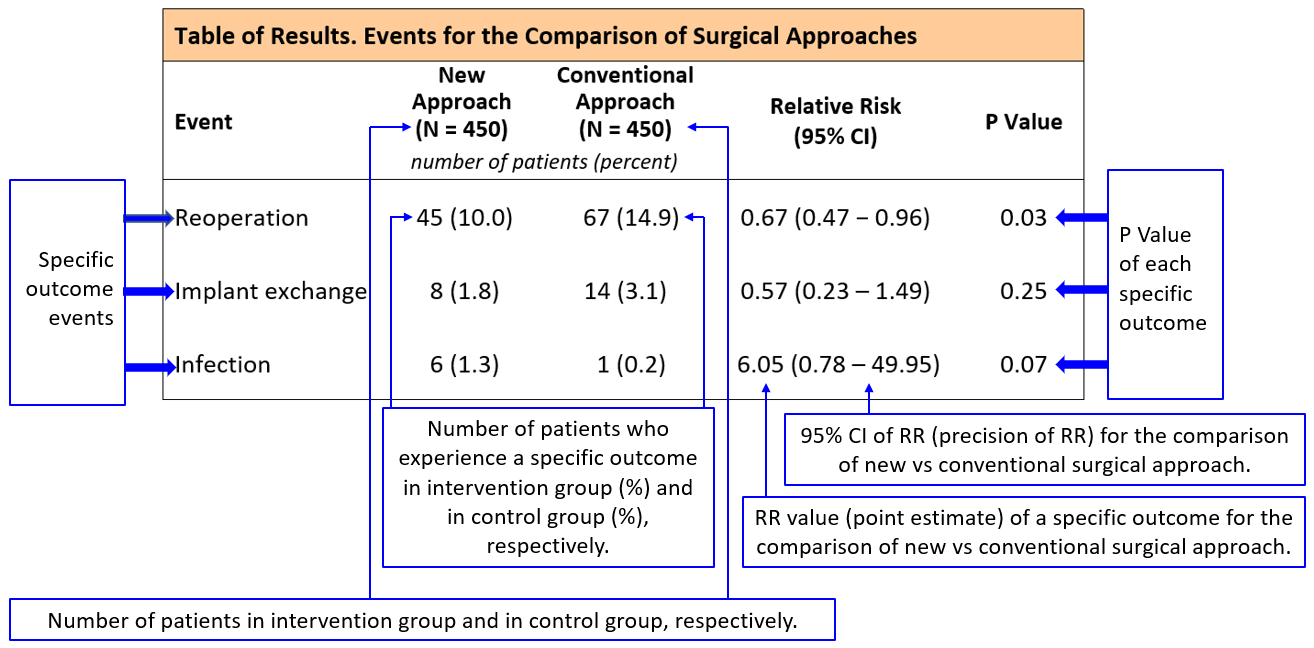
We demonstrate the components of a typical trial table and their meanings in Exhibit 1, using an example of a new surgical approach in comparison with the conventional surgical approach for patients with tibial closed fractures. In this example three dichotomous outcomes are evaluated at 1 year follow-up: reoperation, implant exchange, and infection.
To learn more about 95% CI, click https://myorthoevidence.com/Blog/Show/19.
To learn more about P values, click https://myorthoevidence.com/Blog/Show/16.
Exhibit 1: Anatomy of a Results Table
Category of Measures
Measures of association can be understood as measures of a treatment effect in clinical trials. They fall into two categories, relative difference and absolute difference (Exhibit 2) (Bhandari et al., 2001; Guyatt et al., 2014).
Exhibit 2: Measures of Association in Medical Literature
Measures of Association (Measures of Effect) | |
Relative Difference Measures | Absolute Difference Measures |
Risk Ratio / Relative Risk (RR) Relative Risk Reduction (RRR) or Relative Benefit Increase (RBI) Odds Ratio (OR) Hazard Ratio (HR) | Risk Difference (RD) or Absolute Risk Reduction (ARR) or Absolute Risk Increase (ABI) Number Needed to Treat (NTT) or Number Needed to Harm (NNH) |
Tip 1. RR: All about Risk
RR represents relative risk, risk ratio, or rate ratio. Risk, or absolute risk, is regarded as a measure of an event occurrence and is expressed as the rate of a certain event among participants in a study group.
In the Study to Prospectively evaluate Reamed Intramedullary Nails in Tibial fractures (S[Y1] PRINT Investigators, 2008), we read,
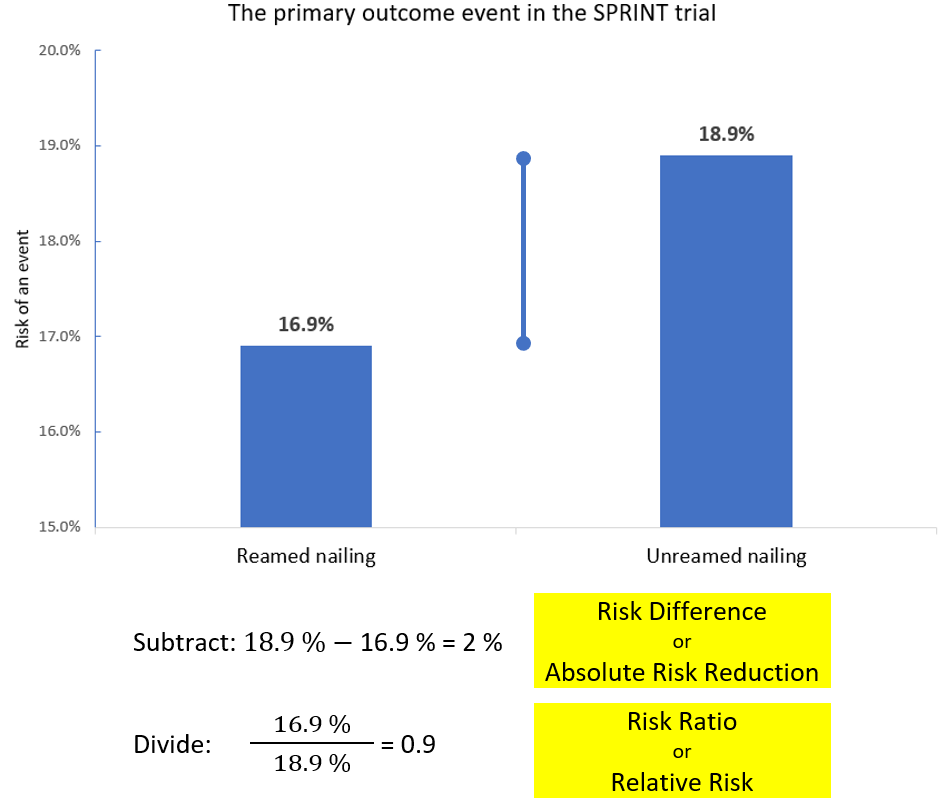
“105 patients (16.9%) in the reamed nailing group and 114 patients (18.9%) in the unreamed nailing group experienced a primary outcome event (relative risk 0.90; 95% CI 0.71-1.15; P=0.40). The primary outcome was defined as a composite including reoperation and / or autodynamization within one year.”
In this trial, there were 622 patients in the reamed nailing and 604 patients in the unreamed nailing group. As shown in the statement, the risk of the primary outcome event (i.e., event rate) in the reamed nailing group was calculated as 105 / 622 = 16.9%. In the same way, the risk of the primary outcome event in the unreamed nailing group was 114 / 604 = 18.9%. Exhibit 3 shows the calculation method of RD (i.e., ARR, difference between the two rates) and RR (by dividing the two rates).
Exhibit 3: Calculation of RD and RR
In plain language, an RR of 0.9 tells us that the risk of primary outcome event (reoperation and / or autodynamization) among those undergoing reamed nailing is nine tenths of those undergoing unreamed nailing approach within one year of follow-up. |
RR is a ratio of rates; therefore, its values are greater than or equal to zero. The closer to 1 an RR value is, the smaller difference it indicates. Exhibit 4 summarizes the meaning of RR values.
Exhibit 4: Meaning of RR and 95% CI values in clinical studies investigating effects of a treatment and predictors of a disease
(in situation of a “bad” outcome, e.g., reoperation and infection)
Meaning | |
RR = 1 or 95% CI of RR includes 1 | Risk is the same in two groups (no association of treatment / exposure and outcome). There is no difference in effect between intervention and control groups. |
RR and 95% CI values > 1 (95% CI does not include 1) | Treatment group has higher risk than control group (possible harmful effect); or Exposure group has higher risk than unexposed group (possible risk factor). |
RR and 95% CI values < 1 (95% CI does not include 1) | Control group has higher risk than treatment group (possible beneficial effect); or Unexposed group has higher risk than exposure group (possible protective factor). |
Notes:
- When a “good” outcome is analysed, e.g., incidence of satisfaction with surgery and incidence of meniscus healing, the meaning of RR values turn to their opposite directions and we change the word “risk” to “proportion”.
- To learn more about 95% CI, click https://myorthoevidence.com/Blog/Show/19.
RR is commonly used to evaluate predictors (prognostic factors, risk factors) of patient outcomes. In an observational study reporting predictors of reoperation after operative management of tibial fractures (Bhandari et al., 2003), we read,
“Multivariate analysis of open vs closed injury showed that the presence of any size open fracture wound (vs closed injury) is one of the predictors of reoperation (relative risk 4.32, 95% CI 1.76 to 11.26).”
In plain language, we would say that the patients with open injuries are 4.32 times more likely to have a reoperation compared to those with closed injuries. The true association is probably ranging from 1.76-fold to 11.26-fold. |
Tip 2. It just takes one step from RD to NNT
What is the RD of 2% telling us (SPRINT trial primary outcome)?
An RD of 2% tells us that in order to prevent the primary outcome events in 2 patients with tibial shaft fractures, you may consider choosing the reamed nailing approach for 100 patients. |
Here is the question: In order to prevent the primary outcome event in 1 patient with tibial shaft fracture, how many patients do you need to treat with a reamed nailing approach?
The NNT is the answer. NNT = 1 / RD (%) = 100 / RD (percent value) = 100 / 2 = 50.
In plain language, an NNT of 50 suggests that, for every 50 patients treated with reamed nailing, the surgeon can prevent 1 primary outcome event (reoperation and / or autodynamization). |
Tip 3. RRR is an alternative expression of RR as a difference in percentage
RRR = 1 - RR
RRR = 1 - 0.9 = 0.1 = 10% (SPRINT trial primary outcome)
In plain language, an RRR of 10% suggests that, the risk of primary outcome event (reoperation and / or autodynamization) receiving reamed nailing is reduced by 10% compared to the unreamed nailing approach. In other words, reamed nailing reduced the risk of primary outcome event by one tenth compared with unreamed nailing. |
Tip 4. HR: Why fuss about survival analysis?
When we calculate the RR, we need to make sure that all the individuals have the same duration of follow-up to evaluate occurrence of an outcome. This requirement is difficult to fulfill, because some patients may enter in a study later than the others, or withdraw from the study before the end of trial. Survival analysis is an appropriate measure, especially in large trials, when patients enter in a study at different time points but end at the same time. Theoretically, HR is the accumulated RR over time and we calculate HRs with statistical softwares when conducting survival analysis. As HR takes into account the timing of an event, its value can be regarded as the measure of association between treatment / exposure and event that incorporate duration of individual patients’ follow-up.
In the trial of Fixation using Alternative Implants for the Treatment of Hip fractures (F[Y2] AITH Investigators, 2017), we read,
“107 of 542 patients (20%) in the sliding hip screw group versus 117 of 537 patients (22%) in the cancellous screws group (hazard ratio [HR] 0.83, 95% CI 0.63–1.09; p=0.18) had reoperations within 24 months.”
In plain language, an HR of 0.83 tells us that, at any point in time, sliding hip screw approach provides 17% risk reduction of reoperation compared to cancellous screws. The true effect probably ranges from 37% lower to 9% higher risk of reoperation. |
Notes: This is an expression of RRR. 1 - 0.83 = 17% for the point estimate; 1 - 0.63 = 0.37 = 37% and 1 - 1.09 = - 0.09 = - 9% for lower and upper limits of the 95% CI.
In the trial of Fluid Lavage of Open Wounds (F[Y3] LOW Investigators, 2015), we read,
“Reoperation occurred in 182 of 1229 patients (14.8%) in the soap group and in 141 of 1218 (11.6%) in the saline group (hazard ratio, 1.32, 95% CI, 1.06 to 1.66; P = 0.01).”
The HR of 1.32 tells us that, at any point in time, soap has a 32% risk increase of reoperation compared to saline as an irrigation solution for open wounds. The true effect probably ranges from 6% to 66% risk increase of reoperation. |
RR and HR are not exactly the same but the understanding of their values is the same, i.e., the closer to 1 an HR (or RR) value is, the smaller difference it indicates, and vice versa.
Tip 5. OR: play around with the same n and N
While RR is the ratio of risks / rates, OR is the ratio of odds that can be expressed as the following formul[Y4] a:
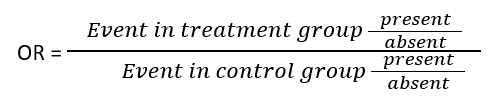
Both RR and OR evaluate the magnitude of treatment effects or risk factors influencing outcome occurrence. OR is usually used in case-control studies, case series, retrospective cohort studies and some statistical models. When the overall event rate in a population is low (which is a common situation in clinical studies), OR is numerically close to RR (Guyatt et al., 2014).
Exhibit 5: Numerical comparison of RR and OR
| Study A 2000 patient study Overall event rate 1.5% | Study B 2000 patient study Overall event rate 37.5% | ||
| N infected | N not infected | N infected | N not infected |
Treatment | 10 | 990 | 250 | 750 |
Control | 20 | 980 | 500 | 500 |
RR | 1% / 2% = 0.5 | 25% / 50% = 0.5 | ||
OR | Odd in treatment group = 10 / 990 =0.01 Odd in control group = 20 / 980 = 0.02 OR = 0.01 / 0.02 = 0.5 | Odd in treatment group = 250 / 750 =0.33 Odd in control group = 500 / 500 = 1 OR = 0.33 / 1 = 0.33 | ||
Exhibit 5 shows examples of two studies with different event rates. In study A with a low overall event rate (30 / 2000 = 1.5%), the value of RR becomes the same as that of OR. However, in study B with a higher event rate (750 / 2000 = 37.5%), RR (=0.5) and OR (=0.33) differ much. We can also find that, when RR and OR differ, OR will always make the treatment appear more effective than the result of RR (the OR, 0.33 is more away from 1 than the RR, 0.5; and more away from 1, the greater effect).
Bottom Line
We need to refer to the 95% CI ([Y5] The 1 Thing You Need to Know When Interpreting Study Results with Confidence!) to understand the results of all the measures when we apply the trial results to clinical practice.
Related ACE Reports:
https://myorthoevidence.com/AceReports/Report/2879
https://myorthoevidence.com/AceReports/Report/9884
https://myorthoevidence.com/AceReports/Report/8216
References
1. Bhandari M, Guyatt GH, Swiontkowski MF. User’s guide to the orthopaedic literature: how to use an article about a surgical therapy. JBJS. 2001 Jun 1;83(6):916-26.
2. Bhandari M, Tornetta P, Sprague S, Najibi S, Petrisor B, Griffith L, Guyatt GH. Predictors of reoperation following operative management of fractures of the tibial shaft. Journal of orthopaedic trauma. 2003 May 1;17(5):353-61.
3. Fixation using Alternative Implants for the Treatment of Hip fractures (FAITH) Investigators. Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial. Lancet. 2017 Apr 15;389(10078):1519-1527.
4. Flow Investigators. A trial of wound irrigation in the initial management of open fracture wounds. New England Journal of Medicine. 2015 Dec 31;373(27):2629-41.
Guyatt G, Rennie D, Meade MO, Cook DJ. Users’ Guide to the Medical Literature: A Manual for Evidence-Based Clinical Practice, 3rd Edition, New York, NY: The McGraw-Hill Companies, Inc. 2014.
5. Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures (SPRINT) Investigators. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. The Journal of Bone and Joint Surgery. American volume. 2008 Dec 1;90(12):2567.
Join the Conversation
Please Login or Join to leave comments.